 Overview OverviewHammer toe is defined as a deformity in the toe where part of the toe is permanently bent downward resembling a hammer. Two Hammer toe related conditions are mallet toe and claw toe which effect different toe joints in slightly different ways. The key difference is that Hammer toes tends to effect the middle joint in the toe (note: not the middle toe, the middle toe joint). The disease is usually associated with the second largest toe but can effect the third or fourth toe as well. Mallet toe effects the uppermost toe joint whereas claw toe is caused by the tow being held in a cramped ?claw-like? position. Causes Footwear can contribute significantly to the development of hammertoes. Shoes that are too small force your toes into a curled position. Over time, your toe tendons adjust to this positioning, causing your toe or toes to hold a hammered shape. Athletes may be especially susceptible, because of the increased forces on the toes from shoes that are too small or tight. Heel elevation in footwear is also problematic, as it causes your toes to be pushed into the shoe?s toe box. Heel elevation additionally contributes to muscle imbalance. A common example of this is when your Achilles tendon-the tendon at the back of your leg that attaches your calf muscles to your heel bone-is too tight, causing the tendons on the top of your foot that attach to your toes to work too hard and hold your toes in an unnatural, elevated position.  Symptoms SymptomsThe most obvious sign of hammertoes are bent toes, other symptoms may include pain and stiffness during movement of the toe. Painful corns on the tops of the toe or toes from rubbing against the top of the shoe's toe box. Painful calluses on the bottoms of the toe or toes. Pain on the bottom of the ball of the foot. Redness and swelling at the joints. Diagnosis The treatment options vary with the type and severity of each hammer toe, although identifying the deformity early in its development is important to avoid surgery. Your podiatric physician will examine and X-ray the affected area and recommend a treatment plan specific to your condition. Non Surgical Treatment Inserts in your shoes can be used to help relieve pressure on the toes from the deformity. Splints/Straps. These can be used to help re-align and stretch your toes and correct the muscle imbalance and tendon shortening. One of the most common types are toe stretchers like the yogatoe. Chiropody. A chiropodist can remove calluses or corns, areas of hard skin that have formed to make the foot more comfortable.Steroid injections can help to reduce pain and inflammation. Surgical Treatment Treatment of a severe hammertoe that has become rigid includes surgery. What is done during the surgery depends on how misshapen and inflexible the toe is. The surgeon may make a cut over your toe and release the tendon by cutting the tendon away from the bone. The surgeon may remove a small piece of bone from the toe. The surgeon may realign the tendons to reposition your toe or fasten the bones with pins. Sometimes the surgeon may have to join the bones in the toe. In this case, you will no longer be able to bend the toe, but the toe will be flat.  Prevention PreventionHammertoe can usually be prevented by wearing shoes that fit properly and give the toes plenty of room. Don?t wear shoes with pointed or narrow toes. Don?t wear shoes that are too tight or short. Don?t wear high-heeled shoes, which can force the toes forward. Choose shoes with wide or boxy toes. Choose shoes that are a half-inch longer than your longest toe. If shoes hurt, don?t wear them.  Overview OverviewA Hammer toe is a deformity that causes your toe to bend or curl downward instead of pointing forward. This deformity can affect any toe on your foot; however, it most often affects the second toe or third toe. Although a hammertoe may be present at birth, it usually develops over time due to wearing ill-fitting shoes or arthritis. In most cases, a hammertoe is treatable. Causes A hammertoe is formed due an abnormal balance of the muscles in the toes. This abnormal balance causes increased pressures on the tendons and joints of the toe, leading to its contracture. Heredity and trauma can also lead to the formation of a hammertoe. Arthritis is another factor, because the balance around the toe in people with arthritis is so disrupted that a hammertoe may develop. Wearing shoes that are too tight and cause the toes to squeeze can also be a cause for a hammertoe to form.  Symptoms SymptomsThe symptoms of a hammer toe are usually first noticed when a corn develops on the top of the toe and becomes painful, usually when wearing tight shoes. There may be a bursa under the corn or instead of a corn, depending on the pressure. Most of the symptoms are due to pressure from footwear on the toe. There may be a callus under the metatarsal head at the base of the toe. Initially a hammer toe is usually flexible, but when longstanding it becomes more rigid. Diagnosis Most health care professionals can diagnose hammertoe simply by examining your toes and feet. X-rays of the feet are not needed to diagnose hammertoe, but they may be useful Hammer toe to look for signs of some types of arthritis (such as rheumatoid arthritis) or other disorders that can cause hammertoe. Non Surgical Treatment Conservative treatment starts with new shoes that have soft, roomy toe boxes. Shoes should be one-half inch longer than your longest toe. For many people, the second toe is longer than the big toe.) Avoid wearing tight, narrow, high-heeled shoes. You may also be able to find a shoe with a deep toe box that accommodates the hammer toe. Or, a shoe repair shop may be able to stretch the toe box so that it bulges out around the toe. Sandals may help, as long as they do not pinch or rub other areas of the foot. Surgical Treatment If conservative treatments fail and your symptoms persist, the doctor may recommend a surgical option to straighten the toe. The procedures used vary greatly, depending upon the reasons for the hammertoe. There are a number of different operations to correct hammertoes, the most common ones involve Soft tissue corrections such as tendon transfers, tendon lengthening, and joint capsule repairs. Digital arthroplasty involves removal of bone from the bent joint to allow the toe to straighten. The temporary use of pins or K-wires may be necessary to keep the toe straight during the healing period. Joint implants are sometimes used to allow for a better range of motion in the toe following surgery. Digital arthrodesis involves the removal of bone from the bent joint and fusing the toe in a straight position. If the corn is due to a bone spur, the most common procedure used is an exostectomy, in which surgically removing it or filing it down removes the bone spur. Because of the possible complications involved with any surgery, one should be sure to understand the risks that may be involved with surgery to correct hammertoes and remove bone spurs.  Prevention PreventionMost cases of hammertoe can be prevented by wearing shoes that fit properly and give the toes plenty of room. Some recommended guidelines include avoid shoes with pointed or narrow toes. Avoid shoes that are too tight or short. Avoid high-heeled shoes, which can force the toes forward. If the shoes hurt, don't wear them. Choose shoes with wide or boxy toes. Choose shoes that are a half-inch longer than your longest toe.
Overview
 Your big toe is the hardest working toe. Every time your foot pushes off the ground, this toe supports most of your body's weight. Because the big toe is so critical to movement, any problem with it can make walking or even standing painful. A bunion (excess or misaligned bone in the joint) is one of the most common big-toe problems. In addition to causing pain, a bunion changes the shape of your foot, making it harder to find shoes that fit. But you don't have to hobble for the rest of your life. Bunions can be treated. With your doctor's help, your feet can feel and look better. Your big toe is the hardest working toe. Every time your foot pushes off the ground, this toe supports most of your body's weight. Because the big toe is so critical to movement, any problem with it can make walking or even standing painful. A bunion (excess or misaligned bone in the joint) is one of the most common big-toe problems. In addition to causing pain, a bunion changes the shape of your foot, making it harder to find shoes that fit. But you don't have to hobble for the rest of your life. Bunions can be treated. With your doctor's help, your feet can feel and look better.Causes Bunions are most widely considered to be due to an imbalance in the forces that is exerted across the joint during walking. The resulting abnormal motion and pressure over the joint, over many years (combined with poor fitting footwear) leads to instability in the joint causing hallux valgus and bunions. Bunions are really only a symptom of faulty foot mechanics and are usually caused by a combination of the way we walk, the foot we inherit and inappropriate footwear use. Symptoms The main problem is usually the pressure of the shoe over the bony prominence, which causes discomfort or pain. Sometimes the skin over the lump becomes red, blistered or infected. The foot may become so broad that it is difficult to get wide enough shoes. The big toe sometimes tilts over so much that it rubs on the second toe, or pushes it up out of place so it presses on the shoe. Also, the big toe does not work as well with a bunion, and the other toes have to take more of the weight of the body as you walk. This can cause pain under the ball of the foot ("metatarsalgia"). Sometimes arthritis develops in the deformed joint, causing pain in the joint. Diagnosis Before examining your foot, the doctor will ask you about the types of shoes you wear and how often you wear them. He or she also will ask if anyone else in your family has had bunions or if you have had any previous injury to the foot. In most cases, your doctor can diagnose a bunion just by examining your foot. During this exam, you will be asked to move your big toe up and down to see if you can move it as much as you should be able to. The doctor also will look for signs of redness and swelling and ask if the area is painful. Your doctor may want to order X-rays of the foot to check for other causes of pain, to determine whether there is significant arthritis and to see if the bones are aligned properly. Non Surgical Treatment In most cases the symptoms of bunions can be reduced or relieved without surgery. Reducing pressure on the bunion is the first step in reducing the pain associated with the condition. Wearing correctly fitting shoes is important in achieving this. A referral to a podiatrist may be made in order to assess the need for special orthotic devices, such as custom-made arch supports and shoe inserts (eg: metatarsal pad or bar). These can help to relieve tension on the base of the big toe and help prevent flat-footedness. Specific exercises and bunion pads available over-the-counter at pharmacies may also be of benefit. Anti-inflammatory medicines can help to ease pain in the short term. Steroid injections may be used to relieve severe pain. If a sufficient reduction in symptoms is not achieved by non-surgical treatment, then surgery may be recommended.  Surgical Treatment If your bunion is symptomatic and causing you persisting and troublesome symptoms then surgery should be considered. There is no correct amount of pain or inconvenience which a bunion may cause which warrants surgery. Symptoms which a bunion causes are generally subjective, and what is a problem in one person?s view will not be a problem in another's. For bunion surgery to be successful (correcting the deformity and losing the symptoms) the mechanical factors driving the deformity should be overcome. Bunion surgery should replace the 1st metatarsal closer to the 2nd thus reducing the width of the foot, and also realigning the tendons and reducing their deforming forces. These principals of bunion surgery are well demonstrated by the following x-rays which shows how a Scarf osteotomy has achieved this aim. Overview
The way your foot rolls when it hits the ground is known as pronation, and if you're a runner, it's essential to know what type of pronator you are. There are three types, normal pronation, overpronation, and underpronation (supination). Figuring out your running pattern will help you buy the right running shoe. Not only will this make running more comfortable, but it can also help prevent future injury. 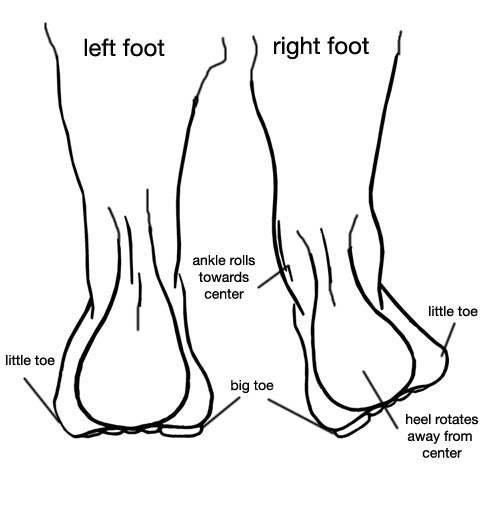 Causes Flat feet don't automatically mean you have a problem. The problem can be divided into a flexible flat foot or rigid flat foot. The rigid flat foot is one that does not change shape when the foot becomes weight bearing. i.e. it does not go through the excessive motion of pronation. Generally speaking this foot does not provide too many problems. The flexible flat foot is the type that when it becomes weight bearing the foot and ankle tends to roll in (pronates) too far. This type of person will often say I have great arches but when I stand up much of this arch disappears as the foot excessively pronates When the foot is excessively pronating and causing problems like sore ankles, feet or knees when standing or exercising then arch support is extremely important to restore the foot structure. Symptoms If you overpronate, your symptoms may include discomfort in the arch and sole of foot. Your foot may appear to turn outward at the ankle. Your shoes wear down faster on the medial (inner) side of your shoes. Pain in ankle, shins, knees, or hips, especially when walking or running.Unfortunately, overpronation can lead to additional problems with your feet, ankles, and knees. Runners in particular find that overpronation can lead to shin splints, tarsal tunnel syndrome, plantar fasciitis, compartment syndrome, achilles tendonitis, bunions (hallux valgus) patello femoral pain syndrome, heel spurs, metatarsalgia. You do not have to be a runner or athlete to suffer from overpronation. Flat feet can be inherited, and many people suffer from pain on a day-to-day basis. Flat feet can also be traumatic in nature and result from tendon damage over time. Wearing shoes that do not offer enough arch support can also contribute to overpronation. Diagnosis So, how can you tell if you have overpronation, or abnormal motion in your feet, and what plantar fasciitis treatment will work to correct it? Look at your feet. While standing, do you clearly see the arch on the inside of your foot? If not, and if the innermost part of your sole touches the floor, then your feet are overpronated. Look at your (running/walking) shoes. If your shoes are more worn on the inside of the sole in particular, then pronation may be a problem for you. Use the wet foot test. Wet your feet and walk along a section of pavement, then look at the footprints you leave behind. A normal foot will leave a print of the heel connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot. 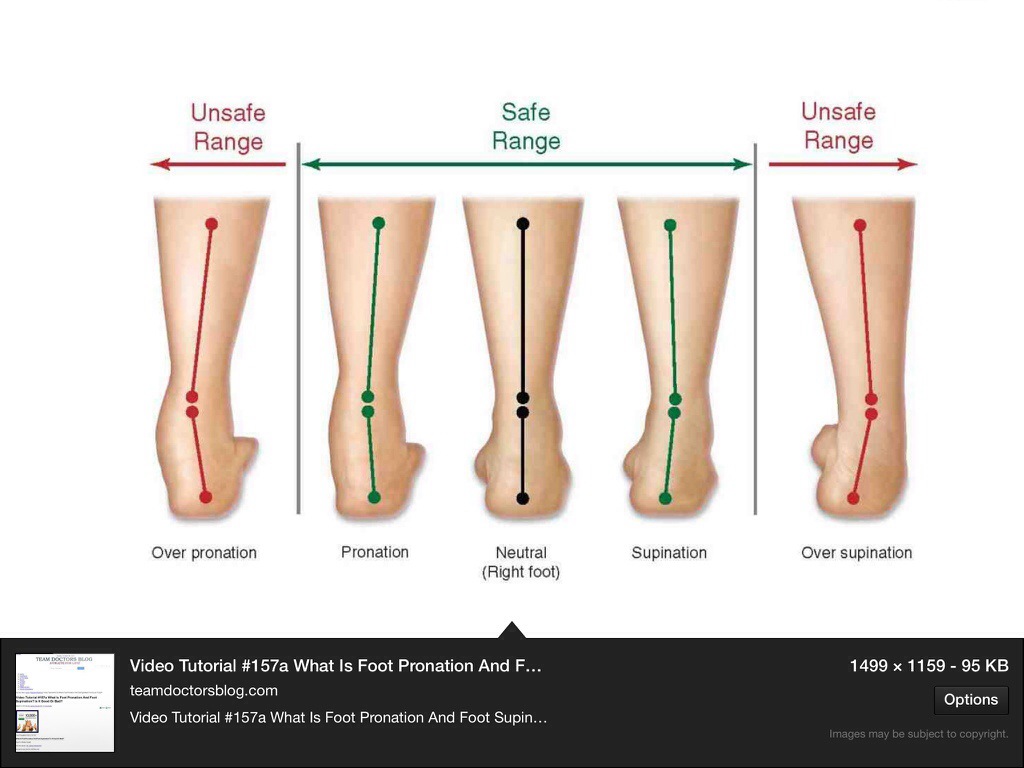 Non Surgical Treatment Over-pronation and the problems that go with it are treated with shoe inserts called arch supports or orthotics. You can buy orthotics at a pharmacy or athletic shoe store or they can be custom made. Make sure the arch supports are firm. If you can easily bend them in half, they may be too flexible. Prevention Strengthen the glutes to slow down the force of the foot moving too far inward. Most individuals who over-pronate have weak glute muscles and strengthening this area is a must. A simple exercise to strengthen glutes is lateral tube walking across a field/court/room. Place a lateral stretch band around your ankles and move your leg sideways while keeping your feet forward. Overview
Sever?s disease (sometimes called Sever disease) is a common cause of heel pain, particularly in the young and physically active. It usually develops just before puberty. Boys are slightly more prone to this condition than girls. Physiotherapy can help manage the symptoms of Sever?s disease so that the young person can continue to take part in physical activity. Another name for Sever?s disease is calcaneal apophysitis. Causes The calcaneal apophysis develops as an independent center of ossification (possibly multiple). It appears in boys aged 9-10 years and fuses by age 17 years, it appears in girls at slightly younger ages. During the rapid growth surrounding puberty, the apophyseal line appears to be weakened further because of increased fragile calcified cartilage. Microfractures are believed to occur because of shear stress leading to the normal progression of fracture healing. This theory explains the clinical picture and the radiographic appearance of resorption, fragmentation, and increased sclerosis leading to eventual union. The radiographs showing fragmentation of the apophysis are not diagnostic, because multiple centers of ossification may exist in the normal apophysis, as noted. However, the degree of involvement in children displaying the clinical symptoms of Sever disease appears to be more pronounced. In a study of 56 male students from a soccer academy, of whom 28 had Sever disease and 28 were healthy control subjects, findings suggested that higher heel plantar pressures under dynamic and static conditions were associated with Sever disease, though it was not established whether the elevated pressures predisposed to or resulted from the disease. Gastrocnemius ankle equinus also appeared to be a predisposing factor. Symptoms As a parent, you may notice your child limping while walking or running awkwardly. If you ask them to rise onto their tip toes, their heel pain usually increases. Heel pain can be felt in one or both heels in Sever's disease. Diagnosis A doctor can usually tell that a child has Sever's disease based on the symptoms reported. To confirm the diagnosis, the doctor will probably examine the heels and ask about the child's activity level and participation in sports. The doctor might also use the squeeze test, squeezing the back part of the heel from both sides at the same time to see if doing so causes pain. The doctor might also ask the child to stand on tiptoes to see if that position causes pain. Although imaging tests such as X-rays generally are not that helpful in diagnosing Sever's disease, some doctors order them to rule out other problems, such as fractures. Sever's disease cannot be seen on an X-ray. Non Surgical Treatment The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Overview
 The Achilles tendon is the soft tissue located in the heel which connects calf muscle to the heel bone allowing the body to perform certain activities such as rising on the tip toes and pushing off when running or walking. Achilles tendon tears occur when the tendon becomes torn through excessive pressure put on the area which the tendon is unable to withstand. Tears are most commonly found when suddenly accelerating from a standing position and therefore is often seen in runners and athletes involved in racquet sports. A tear can also occur when a continuous force is being put on the heel through prolonged levels of activity and overuse however this can also occur as a result of sudden impact or force to the area common in contact sports such as rugby and hockey. Although Achilles tendon tears can range in their severity, a rupture is the most serious form of tear and involves a completely torn tendon. This injury is more common in patients in their 30?s and 40?s. The Achilles tendon is the soft tissue located in the heel which connects calf muscle to the heel bone allowing the body to perform certain activities such as rising on the tip toes and pushing off when running or walking. Achilles tendon tears occur when the tendon becomes torn through excessive pressure put on the area which the tendon is unable to withstand. Tears are most commonly found when suddenly accelerating from a standing position and therefore is often seen in runners and athletes involved in racquet sports. A tear can also occur when a continuous force is being put on the heel through prolonged levels of activity and overuse however this can also occur as a result of sudden impact or force to the area common in contact sports such as rugby and hockey. Although Achilles tendon tears can range in their severity, a rupture is the most serious form of tear and involves a completely torn tendon. This injury is more common in patients in their 30?s and 40?s.Causes The exact cause of Achilles tendon ruptures is hard to say. It can happen suddenly, without warning, or following an Achilles tendonitis . It seems that weak calf muscles may contribute to problems. If the muscles are weak and become fatigued, they may tighten and shorten. Overuse can also be a problem by leading to muscle fatigue . The more fatigued the calf muscles are, the shorter and tighter they will become. This tightness can increase the stress on the Achilles tendon and result in a rupture. Additionally, an imbalance of strength of the anterior lower leg muscles and the posterior lower leg muscles may also put an athlete at risk for an injury to the Achilles tendon. An Achilles tendon rupture is more likely when the force on the tendon is greater than the strength of the tendon. If the foot is dorsiflexed while the lower leg moves forward and the calf muscles contract, a rupture may occur. Most ruptures happen during a forceful stretch of the tendon while the calf muscles contract. Other factors that may increase the risk of Achilles tendon rupture include. Tight calf muscles and/or Achilles tendon. Change in running surface eg: from grass to concrete. Incorrect or poor footwear. A change of footwear eg: from heeled to flat shoes. It is thought that some medical conditions, such as gout, tuberculosis and systemic lupus erythematosus, may increase the risk of Achilles tendon rupture. Symptoms A classic sign of an Achilles tendon rupture is the feeling of being hit in the Achilles are. There is often a "pop" sound. There may be little pain, but the person can not lift up onto his toes while weight bearing. Diagnosis In diagnosing an Achilles tendon rupture, the foot and ankle surgeon will ask questions about how and when the injury occurred and whether the patient has previously injured the tendon or experienced similar symptoms. The surgeon will examine the foot and ankle, feeling for a defect in the tendon that suggests a tear. Range of motion and muscle strength will be evaluated and compared to the uninjured foot and ankle. If the Achilles tendon is ruptured, the patient will have less strength in pushing down (as on a gas pedal) and will have difficulty rising on the toes. The diagnosis of an Achilles tendon rupture is typically straightforward and can be made through this type of examination. In some cases, however, the surgeon may order an MRI or other advanced imaging tests. Non Surgical Treatment Once a diagnosis of Achilles tendon rupture has been confirmed, a referral to an orthopaedic specialist for treatment will be recommended. Treatment for an Achilles tendon rupture aims to facilitate the torn ends of the tendon healing back together again. Treatment may be non-surgical (conservative) or surgical. Factors such as the site and extent of the rupture, the time since the rupture occurred and the preferences of the specialist and patient will be considered when deciding which treatment will be undertaken. Some cases of rupture that have not responded well to non-surgical treatment may require surgery at a later stage. The doctor will immobilise the ankle in a cast or a special hinged splint (known as a ?moon boot?) with the foot in a toes-pointed position. The cast or splint will stay in place for 6 - 8 weeks. The cast will be checked and may be changed during this time.  Surgical Treatment Surgery is the most common treatment for this condition. An incision is made in the lower leg and the tendon is sewn back together. A cast, splint, walking boot, or brace is worn for 6-8 weeks. One of the benefits of surgery is that it lowers the risk of re-rupturing the tendon. Surgery may also be a better option if you are athletic. Prevention Good flexibility of the calf muscles plays an essential role in the prevention of Achilles tendon injuries. It is also important to include balance and stability work as part of the training programme. This should include work for the deep-seated abdominal muscles and for the muscles that control the hip. This might at first appear odd, given the fact that the Achilles are a good distance from these areas, but developing strength and control in this area (core stability) can boost control at the knee and ankle joints. Training errors should be avoided. The volume, intensity and frequency of training should be monitored carefully, and gradually progressed, particularly when introducing new modes of training to the programme. Abrupt changes in training load are the primary cause of Achilles tendinopathy. Overview
Leg length discrepancies are differences between the lengths of your legs. Not only can the actual difference vary from person to person but also how much it affects daily life. Small discrepancies often go unnoticed and do not need to be treated. Larger differences may affect posture or cause a limp during walking. The discrepancy may be from the upper leg bone (femur) or the lower leg bone (tibia).  Causes There are many causes of leg length discrepancy. Structural inequality is due to interference of normal bone growth of the lower extremity, which can occur from trauma or infection in a child. Functional inequality has many causes, including Poliomyelitis or other paralytic deformities can retard bone growth in children. Contracture of the Iliotibial band. Scoliosis or curvature of the spine. Fixed pelvic obliquity. Abduction or flexion contraction of the hip. Flexion contractures or other deformities of the knee. Foot deformities. Symptoms Back pain along with pain in the foot, knee, leg and hip on one side of the body are the main complaints. There may also be limping or head bop down on the short side or uneven arm swinging. The knee bend, hip or shoulder may be down on one side, and there may be uneven wear to the soles of shoes (usually more on the longer side). Diagnosis Asymmetry is a clue that a LLD is present. The center of gravity will shift to the short limb side and patients will try to compensate, displaying indications such as pelvic tilt, lumbar scoliosis, knee flexion, or unilateral foot pronation. Asking simple questions such as, "Do you favor one leg over the other?" or, "Do you find it uncomfortable to stand?" may also provide some valuable information. Performing a gait analysis will yield some clues as to how the patient compensates during ambulation. Using plantar pressure plates can indicate load pressure differences between the feet. It is helpful if the gait analysis can be video-recorded and played back in slow motion to catch the subtle aspects of movement. Non Surgical Treatment To begin a path torwards a balanced foundation and reduce pain from leg length discrepancy, ask your doctor about these Functional Orthotics and procedures. Functional Orthotics have been shown to specifically reduce pain from leg length inequality, support all three arches of the foot to create a balanced foundation, maximize shock absorption, add extra propulsion, and supply more stability, enable posture correction and long-term preventive protection. Will improve prolonged effectiveness of chiropractic adjustments. Shoe or heel Lifts, Correct the deficiencies that causes imbalances in the body.  Surgical Treatment Differences of an inch-and-a-half to two inches may require epiphysiodesis (adjusting the growth of the longer side) or acute shortening of the other side. Differences greater than 2.5 inches usually require a lengthening procedure. The short bone is cut and an external device is applied. Gradual lengthening is done over months to allow the muscles and nerves accommodate the new length.
Overview
Posterior tibial tendon dysfunction (PTTD) is an inflammation and / or overstretching of the posterior tibial tendon in the foot. An important function of the posterior tibial tendon is to help support the arch. But in PTTD, the tendon?s ability to perform that job is impaired, often resulting in a flattening of the foot. PTTD is often called ?adult-acquired flatfoot? because it is the most common type of flatfoot developed during adulthood. Although this condition typically occurs in only one foot, some people may develop it in both feet. PTTD is usually progressive, which means it will keep getting worse-especially if it isn?t treated early. This differs from flexible flatfoot because flexible flatfoot typically begins in childhood or adolescence and continues into adulthood. It usually occurs in both feet and generally progresses in severity throughout the adult years. As the deformity worsens, the soft tissues (tendons and ligaments) of the arch may stretch or tear and become inflamed. The term ?flexible? means that while the foot is flat when standing (weight bearing), the arch returns when not standing. In the early stages of flexible flatfoot arthritis is not restricting motion of the arch and foot, but in the later stages arthritis may develop to such a point that the arch and foot become stiff.  Causes As the name suggests, adult-acquired flatfoot occurs once musculoskeletal maturity is reached, and it can present for a number of reasons, though one stands out among the others. While fractures, dislocations, tendon lacerations, and other such traumatic events do contribute to adult-acquired flatfoot as a significant lower extremity disorder, as mentioned above, damage to the posterior tibial tendon is most often at the heart of adult-acquired flatfoot. One study further elaborates on the matter by concluding that ?60% of patients [presenting with posterior tibial tendon damage and adult-acquired flatfoot] were obese or had diabetes mellitus, hypertension, previous surgery or trauma to the medial foot, or treatment with steroids?. Symptoms Depending on the cause of the flatfoot, a patient may experience one or more of the different symptoms here. Pain along the course of the posterior tibial tendon which lies on the inside of the foot and ankle. This can be associated with swelling on the inside of the ankle. Pain that is worse with activity. High intensity or impact activities, such as running, can be very difficult. Some patients can have difficulty walking or even standing for long periods of time. When the foot collapses, the heel bone may shift position and put pressure on the outside ankle bone (fibula). This can cause pain on the outside of the ankle. Arthritis in the heel also causes this same type of pain. Patients with an old injury or arthritis in the middle of the foot can have painful, bony bumps on the top and inside of the foot. These make shoewear very difficult. Occasionally, the bony spurs are so large that they pinch the nerves which can result in numbness and tingling on the top of the foot and into the toes. Diabetics may only notice swelling or a large bump on the bottom of the foot. Because their sensation is affected, people with diabetes may not have any pain. The large bump can cause skin problems and an ulcer (a sore that does not heal) may develop if proper diabetic shoewear is not used. Diagnosis In the early stages of dysfunction of the posterior tibial tendon, most of the discomfort is located medially along the course of the tendon and the patient reports fatigue and aching on the plantar-medial aspect of the foot and ankle. Swelling is common if the dysfunction is associated with tenosynovitis. As dysfunction of the tendon progresses, maximum pain occurs laterally in the sinus tarsi because of impingement of the fibula against the calcaneus. With increasing deformity, patients report that the shape of the foot changes and that it becomes increasingly difficult to wear shoes. Many patients no longer report pain in the medial part of the foot and ankle after a complete rupture of the posterior tibial tendon has occurred; instead, the pain is located laterally. If a fixed deformity has not occurred, the patient may report that standing or walking with the hindfoot slightly inverted alleviates the lateral impingement and relieves the pain in the lateral part of the foot. Non surgical Treatment Initial treatment is based on the degree of deformity and flexibility at initial presentation. Conservative treatment includes orthotics or ankle foot orthoses (AFO) to support the posterior tibial tendon (PT) and the longitudinal arch, anti-inflammatories to help reduce pain and inflammation, activity modification which may include immobilization of the foot and physical therapy to help strengthen and rehabilitate the tendon.  Surgical Treatment Types of surgery your orthopaedist may discuss with you include arthrodesis, or welding (fusing) one or more of the bones in the foot/ankle together. Osteotomy, or cutting and reshaping a bone to correct alignment. Excision, or removing a bone or bone spur. Synovectomy, or cleaning the sheath covering a tendon. Tendon transfer, or using a piece of one tendon to lengthen or replace another. Having flat feet is a serious matter. If you are experiencing foot pain and think it may be related to flat feet, talk to your orthopaedist. |
